


























Lower Urinary Tract
The bladder is comprised of the body and the trigone and normally serves to store urine at low pressures and effectively contract to urinate (7). The bladder is composed of an inner transitional epithelium, a multilayer muscular wall, and an outer serosal covering. The exact dimensions and configuration of the bladder vary considerably depending on degree of distention, prolapse, or other pathology. The bladder base and urethra rest on the anterior vaginal wall (1). The bladder is an extraperitoneal organ covered by peritoneum at the dome superiorly and posteriorly.
The peritoneum then reflects onto the anterior vagina and uterus, forming the vesicouterine pouch, and continues over the posterior uterus and onto the rectum, creating the rectouterine space or pouch of Douglas (Fig. 10) (3). The peritoneum in the rectouterine space may herniate into the posterior vagina, resulting in an enterocele.
The ureter is a continuation of the renal collecting system and transports urine from the kidney to the bladder (8). The ureter courses inferiorly and medially; below the inferior border of the sacrum, the ureter is referred to as the lower, distal, or pelvic ureter.
The position of the distal ureter can be affected by bladder distention or significant prolapse, and it is susceptible to injury during pelvic reconstruction. The ureter crosses anterior to the common iliac vessels at the bifurcation medial to the ovarian vessels. The course of the ureter is retroperitoneal and runs deep to the base of the broad ligament before traveling through the cardinal ligament, where the ureter passes underneath the uterine artery (Fig. 11) (3). The ureter is located in the anterior vaginal wall before entering the bladder and is usually 1.5 cm superolateral to the cervix (1).
Fig. 10. Peritoneal cleavage planes. (From ref. 3.)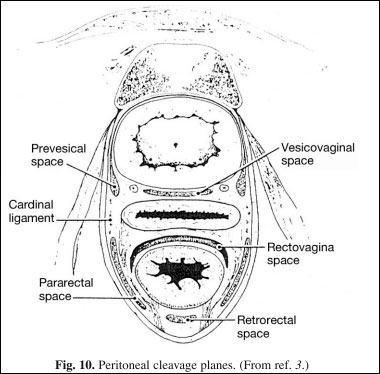
The female urethra is approx 4 cm in length and extends from the bladder neck to the external urethral meatus (1). As mentioned, the midportion of the urethra is attached to the inferior pubis by the pubourethral ligaments. The ligaments divide the urethra into proximal and distal halves; the external sphincter is just distal to the ligaments.
The urethra is typically divided into three portions: proximal, mid, and distal. The proximal urethra is responsible for passive continence. The midportion, which contains the rhabdosphincter, is responsible for passive and active continence. The distal one-third is principally a conduit and, if damaged or resected, usually does not have an impact on continence. The epithelium of the urethra varies proximal to distal, transitional to non-keratinized squamous epithelium, respectively. Many small glands communicate with the urethra and may be a source of urethral diverticula.
The urethra is bordered laterally by two small labia, which contain minor vestibular glands. The Skene ducts open on the inner aspect of these labia and when inflamed can be palpated on the distal anterior vaginal wall as a suburethral mass (3).
The mechanism of continence is multifactorial. Innate properties of the urethra provide a measure of control. The urethral epithelium has many infoldings, which result in a mucosal seal (Fig. 12).
{pagebreak}
The surrounding vascular spongiosum and outer musculofascial layer provide additional compression of the urethra.
Fig. 11. Course of the ureter. (From ref. 3.)
The urethropelvic ligaments provide passive and active support. They suspend the bladder neck and urethra in a higher retropubic position than the more dependent bladder base, creating a valvular effect. During increased activity of the LAG, the ligaments are drawn laterally, increasing compression of the urethra and thereby augmenting continence. Finally, the urethral striated sphincter provides resting tone, contributing to the closing forces of the urethra, and allows for reflex and voluntary urinary control.
The ability to store urine safely and effectively and volitionally void at desired times is a complex process involving the central nervous system and an intact spinal cord.
Innervation of the bladder and urethra is briefly reviewed as it is pertinent to urinary continence (Fig. 13). The urinary system is regulated by autonomic and motor neurons.
The sympathetic nerves arise from the thoracolumbar region (T10-L2) and are carried via the hypogastric nerve, which mediates storage. The parasympathetic nerves originate from the sacral cord (S2-S4), are carried via the pelvic nerve, and facilitate detrusor contraction and voiding. The pudendal nerve, as described in the section on pelvic circulation, also originates from the sacral cord and innervates the urethral rhabdosphincter.
Fig. 12. Urethral histology. E, urethral epithelium; S, surrounding vascular spongiosum; M, outer
musculofascial layer.
Afferent or sensory fibers, which are important during the storage phase, are carried via the pelvic, hypogastric, and pudendal nerves (9).
{pagebreak}
Genital Structures
The uterus is a fibromuscular organ with dimensions and exact orientation that vary considerably depending on hormonal status, age, and parity (3). It is comprised of two parts, an upper muscular corpus and a lower fibrous cervix. The uterus is lined by a unique epithelium, the endometrium. The external cervical os is lined by squamous epithelium and more proximally by columnar epithelium.
The uterus and cervix are supported by surrounding ligaments and fascia (Fig. 14). The cardinal ligaments are dense, triangular condensations of pelvic fascia that originate from the pelvic sidewall and insert into the lateral aspects of a fascial ring encircling the uterine cervix. The cardinal ligaments support the uterus and vaginal apex and, as mentioned, fuse with the pubocervical fascia, providing support for the bladder base (2).
Fig. 13. Bladder and urethral innervation and mechanism of continence. (From ref. 17.)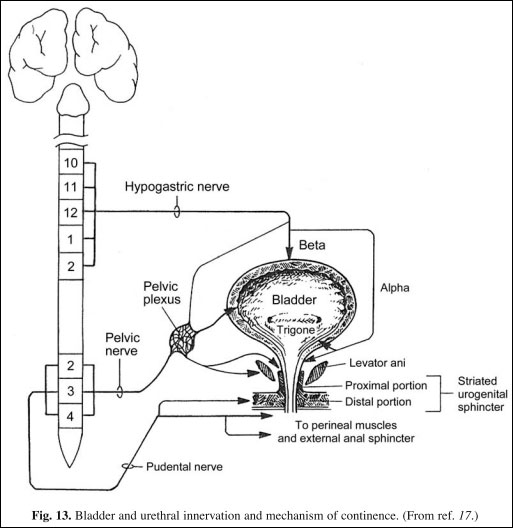
The cardinal ligaments fuse posteriorly with the uterosacral (sacrouterine) ligaments, which stabilize the uterus, cervix, and upper vagina posteriorly to the sacrum. In addition, the broad ligaments are fascial condensations covered by anterior and posterior sheets of peritoneum, which provide lateral support for the more superior portion of the uterus. Many important structures travel within the broad ligament, the fallopian tubes, the round and ovarian ligaments, and the uterine and ovarian vessels. The uterine arteries enter near the junction of the corpus and the cervix; however, this position varies considerably (Fig. 11) (3).
Fig. 14. Schematic diagram of normal uterine support. (From ref. 7.)
The vagina is a hollow viscus with shape that is determined by the structures that surround it. The vagina receives blood supply from downward branches of the uterine artery and vaginal branches of the internal iliac (3). It is made up of an inner epithelium layer, a stratified squamous epithelium, an inner muscular layer, and an outer fibrous layer. The upper vagina is maintained in a nearly horizontal axis by fascial support and inferiorly by the LAG shelf on which it is resting (Fig. 15). When this orientation is altered postpartum or iatrogenically, vaginal prolapse may occur (2). Maintaining functional depth and an adequate hiatus are important considerations in women who desire future sexual activity.
—-
Melissa Fischer, MD, Priya Padmanabhan, MD, and Nirit Rosenblum, MD
—-
{embed=“ref/1”}



